SARC-F, G8, and Distress Screening Belong Inside the Intake Workflow
Known questionnaires create clinical signals only when answers, categories, scoring context, and review stay connected to the patient workflow.

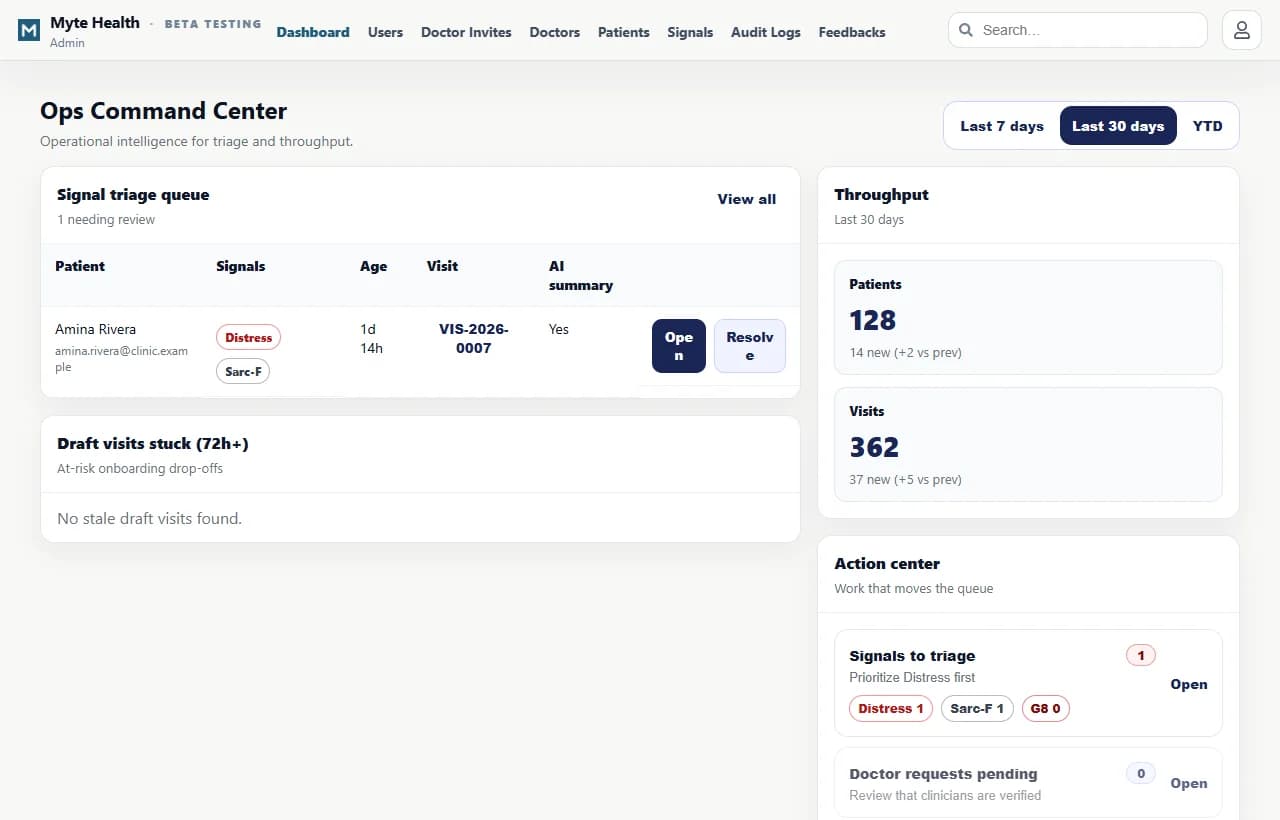
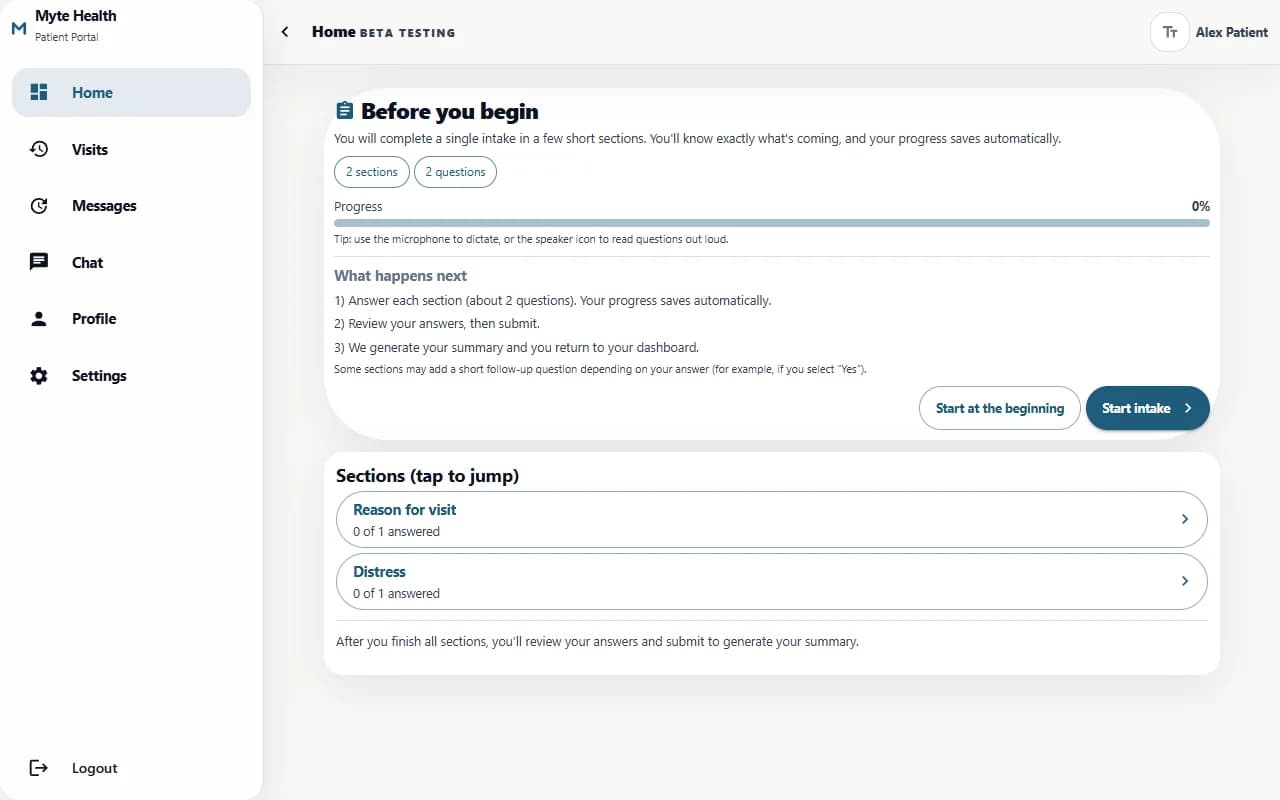
The operator moment
A patient completes intake before the consultation. The clinic needs more than completed forms. It needs to know which answers matter, which signals require attention, and how the doctor will review the information without wasting time.
The hidden cost
The hidden cost of disconnected forms is review friction. Staff collect answers, but clinicians still have to interpret scattered results, re-open documents, or ask patients to repeat information. Structure should reduce that load.
A generic form tool can collect questionnaire answers. A clinical intake system must preserve categories, answer history, patient context, review state, doctor assignment, and final consultation path.
What changes when the system is owned
Workflow map
How to read the proof
Questionnaires should be stored as structured answers with category, timestamp, version, patient link, and review state. AI summaries should reference those records and remain editable by the clinician.
How Myte delivers it
- 1Map the questionnaire set, scoring logic, patient flow, clinical review needs, and admin roles.
- 2Build mobile-first completion with structured answer storage and patient context.
- 3Add signal boards, doctor assignment, summaries, and draft consultation review.
- 4Extend into audit, feedback, search, settings, and additional questionnaire categories.
Buyer checklist
Why this belongs in your operating system
Myte builds questionnaire workflows as clinical operating systems. The goal is to make patient answers useful, reviewable, and connected before the consultation begins.
Approved screenshots and workflow examples that show how the operating model works in practice.
Questions operators ask
Can SARC-F and G8 be digitized?
Yes, but the answers should remain structured and connected to the clinical review path.
What about distress screening?
Distress answers should feed reviewable signals and patient context, not stay inside an isolated form.
Can doctors edit summaries?
Yes. Summaries and drafts should be reviewable and editable before final use.
Can patients complete on mobile?
Yes. The workflow should be mobile-first for patient access.
Does this require AI?
No. The structured workflow is valuable first; AI can assist summaries after the data path is reliable.
Related field notes
Healthcare Intake Software Should Reduce Noise Before the Consultation
A patient intake system becomes valuable when registration, questionnaires, pain maps, voice answers, doctor review, and consultation drafts form one clinical workflow.
Read noteAI Profile Summaries in Healthcare Need an Edit Path
AI summaries help clinicians only when the source answers remain visible and the doctor can review, edit, approve, or ignore the draft.
Read noteHealthcare Operating Systems Need Audit Logs From the First Workflow
Audit logs are not a later compliance accessory. They are how healthcare teams understand access, edits, reviews, finalization, and trust.
Read noteBuild your owned operating system with Myte
Start with one workflow your team already understands, then turn it into software your business owns.