Health Connect Clinical Intake Case Study
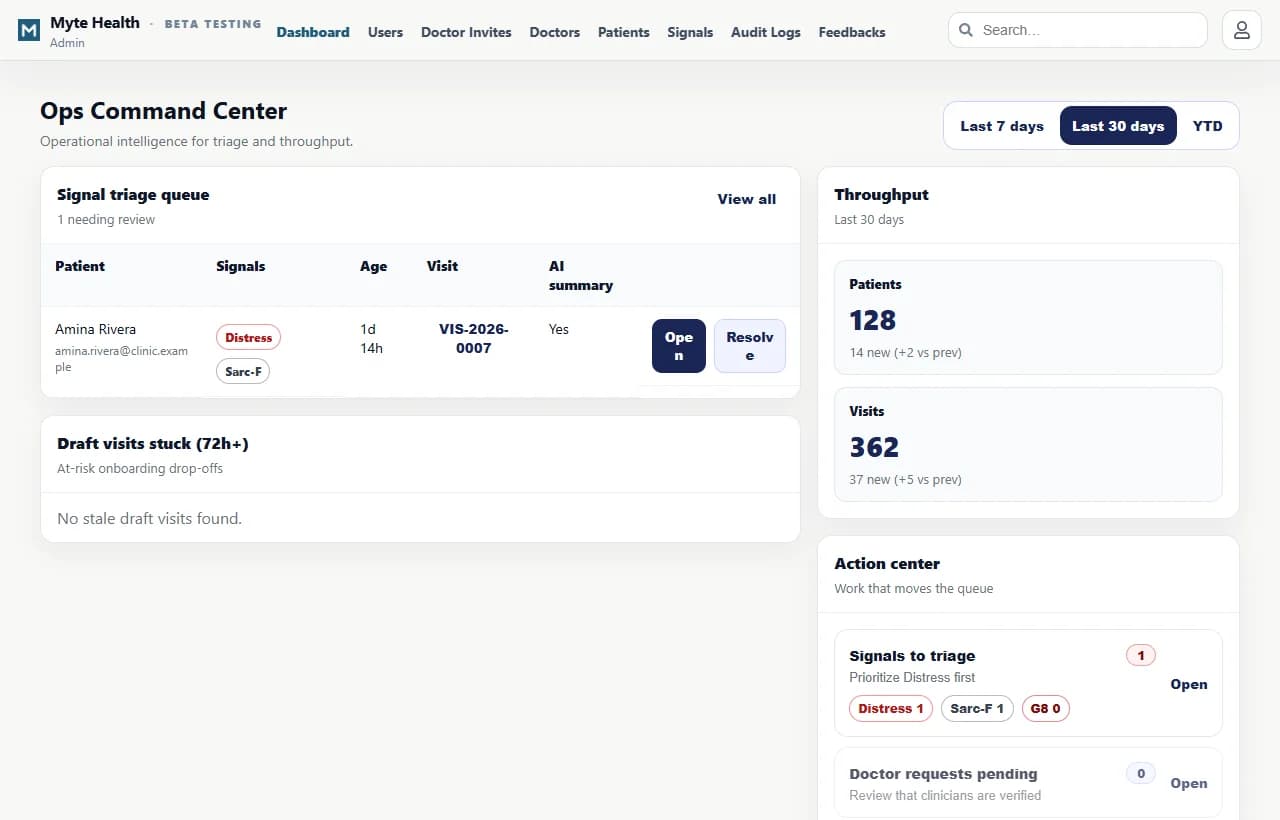
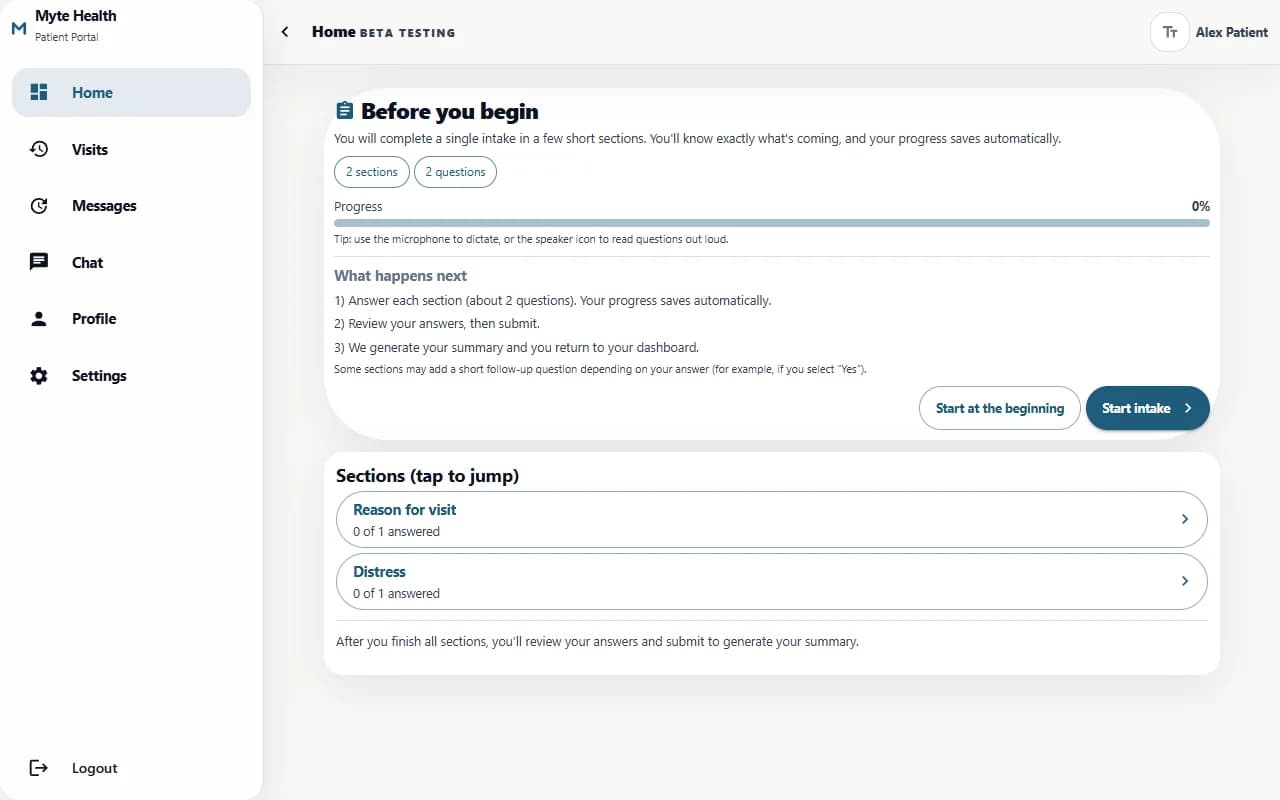
Health Connect shows QR registration, OTP verification, questionnaire categories, Sarc-F, G8, distress signaling, pain map, doctor review, and consultation finalization in one workflow.

The operator moment
A clinician or clinic operator feels the pain when patient context, questionnaire structure, clinical signal review, and consultation readiness has to be reconstructed during active work. The operating question is not whether software can be added. It is whether the business can trust the records, decisions, and next actions when the day is moving quickly.
The hidden cost
The visible cost in a Health Connect clinical intake case study workflow is delay. The deeper cost is that patients, questionnaire answers, clinical signals, assignments, summaries, consultations, and audit logs never become durable enough for reporting, training, ownership, or future AI. The hidden cost compounds because every missing record creates another meeting, another export, another message, or another person rebuilding context from memory.
A form builder or generic portal can help with one piece of Health Connect clinical intake case study, but it does not own the whole workflow or the business-specific decision path. Generic tools may store part of the work, but they rarely model the operating relationship between patients, questionnaire answers, clinical signals, assignments, summaries, consultations, and audit logs, permissions, responsibilities, and accountability.
What changes when the system is owned
Workflow map
How to read the proof
The system should keep source answers structured and make summaries, drafts, edits, and finalization traceable. For Health Connect clinical intake case study, that means QR registration, questionnaire categories, signal board, editable summary, doctor assignment, and final consultation must stay connected to patient registration, Sarc-F, G8, distress signaling, pain maps, summaries, doctor review, drafts, final notes, and audit logs. The architecture should make records, roles, actions, timestamps, and permissions explicit so the system can support reporting, audit, and future AI without losing control.
How Myte delivers it
- 1Map the current workflow, actors, records, language, approval points, and data sources before software decisions are made.
- 2Build the first production release around QR registration, questionnaire categories, signal board, editable summary, doctor assignment, and final consultation so the team can test value quickly.
- 3Train operators with the system open and adjust wording, status, permissions, and responsibilities until the workflow feels native.
- 4Extend reporting, private AI, integrations, documentation, and managed deployment after adoption is visible.
Buyer checklist
Why this belongs in your operating system
Myte builds healthcare workflows that prepare context while keeping clinical review in human hands. The ownership target is QR registration, questionnaire categories, signal board, editable summary, doctor assignment, and final consultation. Myte builds from the workflow foundation up, then supports documentation, training, deployment, and maintenance so ownership becomes practical instead of theoretical.
Approved screenshots and workflow examples that show how the operating model works in practice.
Questions operators ask
What is Health Connect clinical intake case study?
Health Connect clinical intake case study is an owned software approach for Health Connect clinical intake case study. It connects the workflow, records, decisions, and review path instead of leaving the work across disconnected tools.
Who is this for?
It is for teams that already know the work but need patient registration, Sarc-F, G8, distress signaling, pain maps, summaries, doctor review, drafts, final notes, and audit logs to become structured, visible, and easier to maintain.
How is this different from SaaS?
SaaS starts with a vendor workflow. A Myte operating system starts with the business workflow and builds the data model, permissions, deployment, and ownership responsibilities around it.
Can AI be included safely?
Yes, when the data boundary, review path, and deterministic records are designed first. AI should assist the workflow instead of becoming the source of truth.
What is the first step?
Start with one workflow under pressure, define the records and actors, ship a production release, then expand after operators trust it.
Related field notes
Healthcare Intake Software With Doctor Review
Healthcare intake software should structure patient answers while keeping doctors in control of review, edits, and final consultation output.
Read noteAutomate Clinical Intake Without Replacing Clinician Review
Clinical intake automation should structure patient answers, signals, summaries, and drafts while keeping clinician review, edits, and finalization explicit.
Read noteWhat a Union Dispatch Operating System Must Make Visible
Dispatch is not only a queue. It is a trust workflow between contractor requests, staff review, member offers, referrals, and accountable follow-up.
Read noteBuild your owned operating system with Myte
Start with one workflow your team already understands, then turn it into software your business owns.